AESE insight #26
[av_layerslider id='1699']
[av_layerslider id='1697']
[av_section min_height='' min_height_px='95px' padding='no-padding' shadow='no-border-styling' bottom_border='no-border-styling' bottom_border_diagonal_color='#333333' bottom_border_diagonal_direction='' bottom_border_style='' scroll_down='aviaTBscroll_down' custom_arrow_bg='#f37421' id='' color='main_color' custom_bg='#ffffff' src='' attachment='' attachment_size='' attach='scroll' position='top left' repeat='no-repeat' video='' video_ratio='16:9' overlay_opacity='0.5' overlay_color='' overlay_pattern='' overlay_custom_pattern='' av_element_hidden_in_editor='0'][/av_section]
[av_one_full first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_heading heading='AESE Insight #26' tag='h1' style='blockquote modern-quote' size='48' subheading_active='subheading_above' subheading_size='12' padding='15' color='custom-color-heading' custom_font='' av-medium-font-size-title='' av-small-font-size-title='' av-mini-font-size-title='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
AESE Insight > Thinking Ahead
[/av_heading]
[/av_one_full][av_one_full first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_animated_numbers number='3 de dezembro 2020' icon_select='no' icon='ue800' font='entypo-fontello' font_size='' font_size_description='' link='' linktarget='no' color='' custom_color='#444444' admin_preview_bg=''][/av_animated_numbers]
[av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[/av_one_full]
[av_section min_height='' min_height_px='500px' padding='default' shadow='no-shadow' bottom_border='no-border-styling' bottom_border_diagonal_color='#333333' bottom_border_diagonal_direction='scroll' bottom_border_style='scroll' scroll_down='' custom_arrow_bg='' id='' color='main_color' custom_bg='' src='' attach='scroll' position='top left' repeat='no-repeat' video='' video_ratio='16:9' video_mobile_disabled='' overlay_enable='' overlay_opacity='0.5' overlay_color='' overlay_pattern='' overlay_custom_pattern='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av_element_hidden_in_editor='0']
[av_one_third first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_image src='https://www.aese.pt/wp-content/uploads/2020/08/Fátima-Carioca_AESEinsight-10SET.jpg' attachment='62489' attachment_size='full' align='center' styling='' hover='' link='post,5307' target='_blank' caption='' font_size='' appearance='' overlay_opacity='0.4' overlay_color='#000000' overlay_text_color='#ffffff' animation='no-animation' admin_preview_bg=''][/av_image]
[av_image src='https://www.aese.pt/wp-content/uploads/2020/12/Fátima-Carioca_AESEinsight3DEZ.jpg' attachment='68155' attachment_size='full' align='center' styling='' hover='' link='post,5307' target='_blank' caption='' font_size='' appearance='' overlay_opacity='0.4' overlay_color='#000000' overlay_text_color='#ffffff' animation='no-animation' admin_preview_bg=''][/av_image]
[av_heading tag='h3' padding='10' heading='Maria de Fátima Carioca ' color='' style='blockquote modern-quote' custom_font='' size='' subheading_active='subheading_below' subheading_size='15' custom_class='' admin_preview_bg='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av-medium-font-size-title='' av-small-font-size-title='' av-mini-font-size-title='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='']
Dean e Professora de Fator Humano na Organização da AESE Business School
[/av_heading]
[/av_one_third][av_two_third min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_textblock size='' font_color='' color='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
Esta expressão que dá nome a um dos mais recentes livros
[1] de Rosabeth Mosss Kanter, Professora de Liderança em Harvard, sugere que, dada a complexidade dos problemas e a aparente insolubilidade dos mesmos, não chega pensarmos “fora da caixa“ ou, dito de outra forma, mudarmos o paradigma de pensamento. É necessário sair para “fora de portas”. Sair mesmo, literalmente, da nossa casa, da nossa empresa. Sair para a rua, respirar o ar fresco, sentir o sol, o vento e a chuva, conviver com outras pessoas para se deixar inspirar por novas ideias e soluções. Parece simples, e até mesmo agradável, mas só até certo ponto. Naturalmente gostamos de desfrutar da natureza, mas, como seres tribais que essencialmente somos, é sempre um exercício exigente imergir noutras realidades humanas para entender o mundo a partir delas.
[/av_textblock]
[av_toggle_container initial='0' mode='accordion' sort='' styling='' colors='custom' font_color='#f37421' background_color='#dcded9' border_color='']
[av_toggle title='Think outside the building ' tags='']
Sair, também e sobretudo, mentalmente, abandonando os “silos mentais” onde encaixamos os temas. Num mundo interligado, os grandes temas e desafios não se encerram nas instituições e sistemas que os representam, são eles próprios um mundo, um ecossistema. A saúde não se circunscreve aos hospitais ou mesmo ao sistema de saúde, mas pode ser também função de programas alimentares, planos desportivos, ambientes não poluídos, vivência equilibrada do stress no trabalho profissional. De forma semelhante, a educação não é apenas fruto da escola ou do sistema educativo, mas também, e em primeiro lugar, dos pais e da família e, ainda, de todos os grupos, atividades e formações que realizamos durante o chamado período escolar e ao longo de toda a vida. E com os negócios, é fácil constatar que a vida empresarial não se encerra na empresa, mas abrange a comunidade, a relação dinâmica e continuada com clientes, parceiros de negócio, locais e internacionais, e outros
stakeholders.
Em tempos de confinamento, todo este panorama se torna mais evidente: a empresa já não é apenas aquele lugar onde nos reuníamos, mas saiu para fora e está agora, também, em casa de cada um dos colaboradores, e o mesmo com as escolas, com os centros de saúde, com o retalho e muitos outros serviços. E se hoje estas instituições estão nas nossas casas, no pós-pandemia, poderão mesmo acompanhar-nos até onde nós quisermos estar, sem fronteiras.
Vem tudo isto a propósito da importância de pensar “fora de portas” no novo ciclo que se iniciou com a reabertura após o primeiro período de confinamento. Se bem que muitas organizações e empresas nunca pararam, uma grande maioria reduziu a sua atividade ou, mesmo, hibernou. Mas desde junho que, em todos os setores económicos e em muitos países, assistimos à reativação de muitas instituições e empresas. Esta reabertura mostrou, contudo, umas organizações diferentes, com práticas diferentes. Todas estão a operar de forma diferente. Muitos processos complicaram-se e alguns, talvez menos, simplificaram-se. A mudança atinge toda a organização: são os cuidados de higienização e desinfeção, a reorganização das equipas, a digitalização, o redesenho da cadeia de valor, a reinvenção do próprio negócio, a reorientação a novos mercados, os investimentos necessários, etc., etc. As mudanças têm sido muitas, dramáticas (pela sua profundidade e velocidade) e massivas (pela sua abrangência).
Ao olhar para o futuro próximo, num cenário de instabilidade continuada, não há dúvida que a dinâmica de mudança veio para ficar. E é por isso um bom momento para refletir sobre o que resultou até agora, o que aprendemos e as respostas que damos hoje a algumas questões críticas.
Algumas dessas questões críticas que as empresas e instituições em geral se podem colocar são, por exemplo: Como vamos manter a capacidade para consistentemente responder às necessárias mudanças? Existem muitos caminhos diferentes para o futuro, qual é o nosso? Como vamos melhorar o nosso negócio, seja ele um restaurante, um hotel, uma escola, uma empresa, um centro de dia, a partir da situação atual? Tudo irá necessitar muito de investimento, onde o iremos encontrar e em que condições?
Para encontrar respostas, é bom resistir à tentação de nos voltarmos a entrincheirar e, uma vez que as portas se abriram, realmente pensar “fora de portas”, pensar no meio da rua, a partir da realidade quotidiana das pessoas, no meio do mundo. E por 3 razões. Em primeiro lugar, porque encontraremos pessoas e ideias novas, criativas e inovadoras que nunca conheceríamos dentro de casa e que podem muito bem ser oportunas soluções. Depois também, porque assim não perderemos nunca a adesão à realidade e a sua vida própria, permitindo que a nossa razão de ser enquanto empresa evolua e continue a responder às necessidades atuais e futuras. Em terceiro lugar, porque entenderemos melhor a nossa responsabilidade ante a comunidade de pessoas que diretamente impactamos, o mundo e a sociedade em geral.
Em relação a este último ponto, a fragilidade da sustentabilidade atual e o aumento das desigualdades sociais que a pandemia agravou ainda mais, requer a consciência responsável de todos os atores sociais, ou seja, de todos nós. As consequências das nossas ações e decisões afetam-nos e afetam muitos outros à nossa volta, seja no presente seja no futuro.
Assim, e porque de uma crise nunca se sai igual - sai-se pior ou melhor -, o que é mesmo imprescindível é aproveitarmos este momento de transição para fomentar e estimular uma nova cultura de trabalho, de consumo e de convivência social. E que as respostas que encontremos às questões que colocarmos sejam para iniciar processos, marcar caminhos, ampliar horizontes mais além do simples crescimento económico, onde tenha lugar cada pessoa, cada organização e a humanidade inteira.
[1] Think Outside the Building: How Advanced Leaders Can Change the World One Smart Innovation at a Time, HBS, 2020
[/av_toggle]
[/av_toggle_container]
[/av_two_third][av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[/av_section]
[av_section min_height='' min_height_px='500px' padding='default' shadow='no-shadow' bottom_border='no-border-styling' bottom_border_diagonal_color='#333333' bottom_border_diagonal_direction='scroll' bottom_border_style='scroll' scroll_down='' custom_arrow_bg='' id='' color='main_color' custom_bg='' src='' attach='scroll' position='top left' repeat='no-repeat' video='' video_ratio='16:9' video_mobile_disabled='' overlay_enable='' overlay_opacity='0.5' overlay_color='' overlay_pattern='' overlay_custom_pattern='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av_element_hidden_in_editor='0']
[av_one_third first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_image src='https://www.aese.pt/wp-content/uploads/2020/12/Information-into-insight_AESEinsight3DEZ.jpg' attachment='68156' attachment_size='full' align='center' styling='' hover='' link='manually,http://www.strategy-business.com/article/How-companies-can-transform-information-into-insight?gko=d634b' target='_blank' caption='' font_size='' appearance='' overlay_opacity='0.4' overlay_color='#000000' overlay_text_color='#ffffff' animation='no-animation' admin_preview_bg=''][/av_image]
[av_heading tag='h3' padding='10' heading='Anil Khurana, Roger Wery, and Amy Peirce' color='' style='blockquote modern-quote' custom_font='' size='' subheading_active='subheading_below' subheading_size='15' custom_class='' admin_preview_bg='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av-medium-font-size-title='' av-small-font-size-title='' av-mini-font-size-title='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='']
Strategy+Business
[/av_heading]
[/av_one_third][av_two_third min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_textblock size='' font_color='' color='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
As the coronavirus pandemic unfolded, one leading global engineering and technology services company found itself well positioned to meet unprecedented challenges. The firm had kicked off a digital transformation project the year before, including investing in a data and analytics program equipped with advanced tools. For example, it enhanced digital collaboration among engineers using next-generation design software, it automated resource allocation based on skill sets, and it offered business reporting on executive mobile devices.
[/av_textblock]
[av_toggle_container initial='0' mode='accordion' sort='' styling='' colors='custom' font_color='#f37421' background_color='#dcded9' border_color='']
[av_toggle title='How companies can transform information into insight' tags='']
Focus on six organizational elements to build a world-class data and insights capability in the post–COVID-19 world.
A few weeks into the crisis, it became clear that in several major countries in which the company operated, engineering and construction were likely to be considered essential services. The chief information officer began scenario planning. He determined that supporting remote work would be critical in the weeks and months that followed and asked regional leadership and IT teams to accelerate training programs for remote working and the recently launched digital tools. He also asked for a cybersecurity assessment to highlight vulnerabilities and risks, and had his procurement and telecommunications teams contract for additional bandwidth. As a result of these moves, employees were able to seamlessly deliver sophisticated infrastructure and architectural designs to their customers.
Other companies struggled to keep pace with the rate of change. It took the leaders of one global automotive components manufacturer nearly a month to obtain the information and insights needed to make critical staffing changes at various facilities; they later struggled to understand their suppliers’ readiness to restart production. Elsewhere, consumer goods companies lacked the ability to read signals about changing consumer preferences during lockdowns, such as increased demand for kitchen tools and home gym equipment. Some automakers had insufficient information about the financial health of their Tier Two and Tier Three suppliers, hindering efforts to accurately assess risk to assembly operations worth billions of dollars.
Although responses to the crisis and the success of those responses have been varied, a common theme has emerged: Business leaders need an effective way to capture, receive, interpret, and act on information, and to add predictive power and agility to their organization. By ensuring streamlined data availability and using advanced analytics in combining new sources of data to develop proprietary insights, leaders can reveal crises before they wreak havoc, uncover competitive pressures before they threaten market share, and surface opportunities before they become someone else’s advantage. Now is the time for companies to invest in and enhance these data and analytics capabilities as part of their broad digitization efforts.
Companies have recognized this urgency. For example, in a PwC study that surveyed more than 1,600 supply chain executives and decision makers in 33 countries between October and November 2019, 63 percent of Digital Champions — companies ahead of the curve in supply chain excellence — reported that they had already implemented an AI and advanced analytics platform, and another 24 percent said they were piloting such software. (It is worth noting, however, that Digital Champions made up just 9 percent of the overall sample.)
Our own discussions with senior executives at several major companies have revealed that even as they recover from the more immediate effects of the pandemic, leaders are rethinking their competitive strategies and how they will reconfigure their businesses to be more resilient in the future. As they adapt to a new reality and cope with the immense challenges of asymmetry, disruption, age (demographic pressures), polarization, and trust, they will need the ability to manage and draw insights from their information.
At the same time, the advancement and affordability of key technologies has dramatically enhanced the transformative power of information. Consider, for example, the proliferation of connected sensors and infinitely scalable computing and storage capabilities at price points that are compelling for a number of new use cases, coupled with the development of increasingly accessible machine learning (ML) and AI tools. The technology is there, and many companies are already using it. For instance, in manufacturing organizations, IoT solutions that include facial recognition are being used to eliminate “badge swapping,” which puts unapproved people in a tool crib or uncertified operators at the controls of a machine.
Sanjay Ravi, general manager of Microsoft’s automotive industry, observes, “Companies are now getting more real-time signals than ever before from their products, operations, and customers. This real-time information, combined with advanced AI technologies, helps companies gain critical nsights to enable more efficient ways of doing business.”
But bringing this vision to life by building a high-caliber data and information capability can’t be accomplished overnight. In fact, if there is one thing that the coronavirus crisis made clear to many companies, it’s that their information value chain had gaps that could create serious problems during challenging times — gaps not easily overcome. What may not be as clear, then, is how companies should begin their journey to data and analytics excellence.
Para mais artigos da
Strategy+Business>>
[/av_toggle]
[/av_toggle_container]
[/av_two_third][av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[/av_section]
[av_section min_height='' min_height_px='500px' padding='default' shadow='no-shadow' bottom_border='no-border-styling' bottom_border_diagonal_color='#333333' bottom_border_diagonal_direction='scroll' bottom_border_style='scroll' scroll_down='' custom_arrow_bg='' id='' color='main_color' custom_bg='' src='' attach='scroll' position='top left' repeat='no-repeat' video='' video_ratio='16:9' video_mobile_disabled='' overlay_enable='' overlay_opacity='0.5' overlay_color='' overlay_pattern='' overlay_custom_pattern='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av_element_hidden_in_editor='0']
[av_one_third first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_image src='https://www.aese.pt/wp-content/uploads/2020/12/Global-Economy-Is-Recovering-Faster-_AESEinsight_3DEZ.jpg' attachment='68159' attachment_size='full' align='center' styling='' hover='' link='manually,http://hbr.org/2020/11/why-the-global-economy-is-recovering-faster-than-expected' target='_blank' caption='' font_size='' appearance='' overlay_opacity='0.4' overlay_color='#000000' overlay_text_color='#ffffff' animation='no-animation' admin_preview_bg=''][/av_image]
[av_heading tag='h3' padding='10' heading='Philipp Carlsson-Szlezak, Paul Swartz, and Martin Reeves' color='' style='blockquote modern-quote' custom_font='' size='' subheading_active='subheading_below' subheading_size='15' custom_class='' admin_preview_bg='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av-medium-font-size-title='' av-small-font-size-title='' av-mini-font-size-title='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='']
Harvard Business Review
[/av_heading]
[/av_one_third][av_three_fifth min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_textblock size='' font_color='' color='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
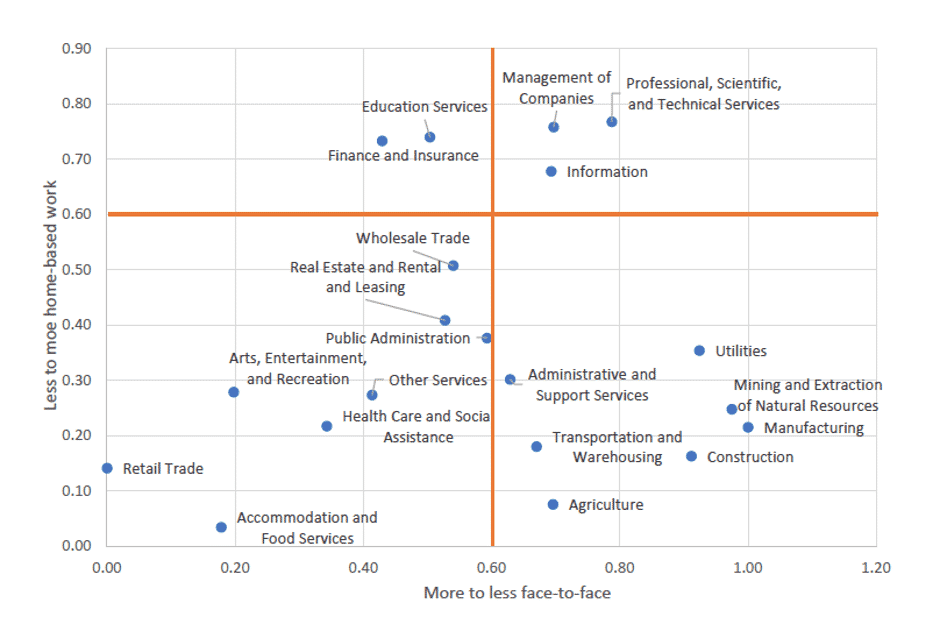
The coronavirus pandemic and ensuing global lockdowns led to fears of a systemic meltdown, but the recovery in the U.S. and around the world has been stronger — and faster — than many predicted. But will it last? Looking at the sectors of the U.S. economy more closely, we can divide it into three parts that were impacted very differently: Sectors that were largely unaffected by Covid (ex: finance and housing); sectors that were impacted by lockdowns, but not social distancing that bounced back relatively quickly (ex: autos and durable goods); and sectors that are won’t be able to meaningfully recover until there’s a vaccine (ex: hospitality, travel). We’ve largely exhausted the “easy” phase of the recovery and the next leg hinges on that third group of sectors.
[/av_textblock]
[av_toggle_container initial='0' mode='accordion' sort='' styling='' colors='custom' font_color='#f37421' background_color='#dcded9' border_color='']
[av_toggle title='Why The Global Economy Is Recovering Faster Than Expected' tags='']
The economic impact of coronavirus continues to surprise. In the spring, previously unimaginable shutdowns pushed economic activity to unimaginable lows. After the initial shock, however, perhaps the biggest surprise has been how fears of systemic meltdown remain unfulfilled — the initial bounce back was far stronger and sooner than expected, and some sectors of the U.S. and other economies have seen complete recoveries to pre-crisis levels of activity.
While the stronger-than-expected recovery aligns with the business experience of many leaders we speak with, they still wonder what drove the gap between expectations and reality — and whether it can last. To answer these questions, we need to look at various recession types and their drivers, how Covid-19 fits in, and what this cycle’s idiosyncrasies are.
Fears Unfulfilled, Hopes Surpassed
As the coronavirus forced the economy into shutdown, a brutal economic contraction unfolded, breaking many (negative) records in the process. Yet, the sustained impact was broadly overestimated — both systemically and cyclically — as the intensity of the shock fueled widespread economic pessimism.
Systemic fears were captured in the popular prediction of a new Great Depression, which would bring sovereign defaults, banking system collapse, and price deflation. Yet after a wobble prices stabilized, sovereign borrowing costs broadly fell across the world despite expansive borrowing, and the banking systems has shown few signs of liquidity problems. (In fact, after hoarding capital banks are looking to return capital again.) The broader systemic fears remain unfulfilled and never looked as perilous as in 2008.
As systemic fears remained unfulfilled, cyclical fears also have proliferated. Unemployment — a cornerstone gauge of economic health — was expected to stay at high levels in the U.S. past the end of 2021. Analysts predicted waves of bankruptcies, a weakening housing market, and a potential collapse after an initial recovery in a “W”-shaped manner.
Yet, here too the surprises have been to the upside. While still unacceptably high, unemployment fell much sooner and faster than thought: By September U.S. unemployment was lower than it was expected to be by the end of 2021. Housing showed remarkable resilience — with prices barely dipping and activity and sales bouncing back to or near the highs since the housing crisis. Many parts of the U.S. economy have returned to pre-crisis levels of activity. Indeed, as the 3Q GDP release last Thursday highlighted, over the last three months growth has been the highest ever recorded. While this does not indicate that the U.S. economy has returned to health or to pre-crisis levels of activity, it is testament to an extraordinarily vigorous rebound after a historically negative second quarter.
These patterns are true around the world: Economic surprise indices, which show an amalgamation of the differences between realized and expected performance, have spiked to record highs everywhere — with the exception for China, where expectations for a full recovery were the baseline.
Why the Covid Recession Outperformed Expectations
While many business leaders have seen these dynamics unfold in real time, they seek to understand the drivers that explain it in order to better see the path ahead. Charting recoveries remains exceptionally difficult (if not as difficult as predicting recessions), but there is value in thinking about the types of recession, their drivers, and impact — as well as about the idiosyncrasies that will shape the remaining recovery path.
There are three dimensions of economic recessions which – when taken together – can help frame the dynamics of recovery. The Covid recession displays distinctive characteristics within this framework that help explain much of what has been on display:
- Recession nature. This captures the underlying force — for example an investment bust, a financial crisis, a policy error or an exogenous shock — that’s afflicting the economy. Despite its brutal intensity, the Covid shock is preferable to an investment bust or a financial crisis that were at the heart of the last two recessions (2001 and 2008/09) because it comes without an overhang of excess investment to work off, which is what delays the onset of recovery and weighs on its trajectory. Indeed, the biggest risk of an exogenous shock is that it morphs into a systemic crisis (traditionally, the fear would be a financial crisis).
- Policy response. This decisively shapes the recovery path and is a clear silver lining of the Covid recession. The speed, feasibility, and effectiveness of fiscal policy has been demonstrated, above all in the U.S. There remains a common misperception that virus caseloads and Covid deaths are strict determinants of economic performance. In reality, the correlation is weak — precisely because a strong economic policy response effectively bridges some of the economic damage from less successful virus control efforts. Think of how U.S. efforts at virus control largely failed relative to other rich nations — in Europe, for example — yet U.S. real growth has still come out ahead. The much bolder U.S. policy effort explains that outcome. Yet, the ultimate impact of policy is to prevent a different type of contagion — household and firm bankruptcies and a wobbly banking system — and this is where structural damage comes in.
- Structural damage. This is the key determinant of a recession’s shape. When a recession leads to a collapse in capital expenditures and pushes workers out of the labor force, an economy’s productive capacity declines. That’s what happened in the U.S. in 2008 as the financial crisis disrupted capital stock growth and made it much harder to return to pre-crisis levels. The Covid recession is more favorable in this respect as there is no “overhang” from the last expansion which did not see excesses in investment or lending that now has to be worked off. Additionally, the fast policy response — unlike in 2008 — contained bankruptcies and drove a strong V-shape recovery in capital goods orders. So far, the Covid recession looks likely to have avoided major structural damage.
It’s quite possible that we were prepared for the worst with the Covid recession because the late and sluggish recovery from the Great Recession is still on our minds. And using the drivers outlined above we can see why: It started as an investment bust that turned into a financial crisis, which in turn impaired financial sector balance sheets and household balance sheets. This was met with a policy response that was quite delayed and kicked in after significant damage was already done. If that serves as in an implicit baseline for how recoveries play out, then the better than expected Covid trajectory should not surprise us.
Can the Covid Recovery Continue to Surprise to the Upside?
To gauge the next leg of recovery we need to go beyond the above drivers – think of them as the necessary foundations for a continued strong recovery – and look at the idiosyncrasies of the Covid recession for sufficient conditions that show how the strength could be delivered.
Looking at the sectors of the U.S. economy more closely, we can divide it into three parts that were impacted very differently given the nature of the virus-driven recession. This suggests the “easy” phase of recovery is exhausted:
- Sectors unaffected by Covid, such as housing and utility consumption, financial services, and off-premise food. Using a household budget as an analogy, you can think of these as “fixed costs” that cannot be reduced easily. This amounts to about 46% of U.S. consumption and never dipped.
- Sectors affected by lockdowns, but not by social distancing, such as autos and other durable goods. These sectors took a big hit from physical lockdowns, but once those were lifted, they bounced back strongly, often fully — and sometimes even exceeding pre-crisis levels. These sectors represent about 16% of the U.S. consumption.
- Sectors that are directly vaccine dependent, such as transportation, recreation, and food service. Some of these sectors bounced back after the lockdown, while others remain unable to meaningfully recover to pre-crisis activity levels because of the risk of exposure to the virus. These sectors represent about 38% of U.S. consumption.
The next leg of a strong recovery thus hinges on that third group of sectors as the recovery potential of the second group is largely exhausted (and the first never dipped). This really moves the question of vaccines front and center. A timeline for the creation of a safe, effective vaccine that provides immunity for a significant time and can be rolled out quickly is fraught with uncertainty. Currently crowdsourced forecasts project a reasonable expectation that a vaccine will become available and meaningfully distributed (i.e. to those most vulnerable and those most at risk of spreading the virus) around Q2 2021.
How It Could All Go Wrong From Here
Neither the necessary nor the sufficient conditions outlined above are guaranteed. A lot can go wrong, and indeed fears of another economic collapse are common in public discourse.
The truly bad scenario is often captured in warnings about a “W-shaped” recession, which would imply another phase of negative growth. In other words, after the collapse (Q2) and the very strong bounce (Q3) we would need Q4 (or Q1 2021) to be a second window of negative growth.
How likely is this scenario? It would almost certainly require a renewed surge of the virus and stringent lockdown that would hamper the second group of sectors. Hospital capacity will prove the ultimate constraint on policy makers’ balancing act between keeping economic activity high and the population safe. While another lockdown is possible, as we’re seeing in Europe, in the U.S. selective shutdowns are more likely given political dynamics, leaving room for growth to stay above zero.
And while positive growth remains our expectation for Q4 and 2021, a host of other risks lingers. A continued failure to extend fiscal stimulus measures could diminish the slope of recovery — or in the extreme turn it negative. A broader political failure — perhaps related to a contested election outcome — is also on the list of risks.
What It Means for Businesses
In times of crisis it’s tempting to be pessimistic and fearful, particular if the drivers are unfamiliar or the risks pose credible systemic threats. However, this inclination to pessimism and retreat also carries risks itself and we should remind ourselves that 14% of firms across all sectors typically grow both revenues and margins during downturns. This is not just idiosyncratic luck — i.e. being in the right sector and seeing a demand boost because of the nature of the crisis — it’s driven by a firm’s ability to see beyond the acute phase of a crisis and exploit its idiosyncrasies to drive differential growth in new areas. While monitoring the overall macro landscape remains important, leaders should not underestimate the importance of measuring, interpreting, and exploiting the dynamics of their own sectors and markets in order to be able to invest and flourish during the recovery and the post-crisis period.
Leia o artigo na integra na Harvard Business Review >>
[/av_toggle]
[/av_toggle_container]
[/av_three_fifth][av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[/av_section]
[av_section min_height='' min_height_px='500px' padding='default' shadow='no-shadow' bottom_border='no-border-styling' bottom_border_diagonal_color='#333333' bottom_border_diagonal_direction='scroll' bottom_border_style='scroll' scroll_down='' custom_arrow_bg='' id='' color='main_color' custom_bg='' src='' attach='scroll' position='top left' repeat='no-repeat' video='' video_ratio='16:9' video_mobile_disabled='' overlay_enable='' overlay_opacity='0.5' overlay_color='' overlay_pattern='' overlay_custom_pattern='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av_element_hidden_in_editor='0']
[av_one_third first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_image src='https://www.aese.pt/wp-content/uploads/2020/12/Amazon-was-built-for-the-pandemic_AESEinsight_3DEZ.jpg' attachment='68162' attachment_size='full' align='center' styling='' hover='' link='manually,http://fortune.com/2020/05/18/amazon-business-jeff-bezos-amzn-sales-revenue-coronavirus-pandemic/?utm_campaign=%20Futurist%20Gerd%20Leonhard%27s%20latest%20findings%2C%20links%20and%20thoughts&utm_medium=email&utm_source=Revue%20newsletter' target='_blank' caption='' font_size='' appearance='' overlay_opacity='0.4' overlay_color='#000000' overlay_text_color='#ffffff' animation='no-animation' admin_preview_bg=''][/av_image]
[av_heading heading='Brian Dumaine' tag='h3' style='blockquote modern-quote' size='' subheading_active='subheading_below' subheading_size='15' padding='10' color='' custom_font='' av-medium-font-size-title='' av-small-font-size-title='' av-mini-font-size-title='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
Fortune
[/av_heading]
[/av_one_third][av_three_fifth min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_textblock size='' font_color='' color='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
If you were designing a company from scratch that could capitalize on a global crisis, it would probably look a lot like Amazon. A fearsome operating machine that inspires equal measures of dread and admiration throughout the business world, the $280-billion-in-sales tech behemoth can react with the speed of the nimblest startup when challenged. Look no further than the company’s response this year to the coronavirus, which founder and CEO Jeff Bezos described to shareholders in late April as “the hardest time we’ve ever faced.”
[/av_textblock]
[av_toggle_container initial='0' mode='accordion' sort='' styling='' colors='custom' font_color='#f37421' background_color='#dcded9' border_color='']
[av_toggle title='Amazon was built for the pandemic—and will likely emerge from it stronger than ever' tags='']
Amazon’s leadership team recognized early on that the pandemic could be a historically disruptive event. And Bezos, who’d been spending one day a week at his rocket company, Blue Origin, quickly became more involved in Amazon’s operations, meeting daily with his “S” (for senior) team—a group of top executives, many of whom have been with the company for a decade or more. Almost overnight, Amazon ramped up its already massive online retail business to meet a huge surge in orders in the first quarter, as customers hunkered down at home and turned to the web for essential supplies. To bolster its response, the company embarked on an effort to vet and hire 175,000 additional employees.
The rapid mobilization paid off. For the three months ended in March, Amazon brought in $75.4 billion in revenue—a 26% gain over 2019. Sales at Amazon Web Services, the company’s cloud-computing business, crossed $10 billion in a quarter for the first time, as customers like streaming entertainment giant Netflix, videoconference sensation Zoom, and workplace-collaboration tool Slack experienced huge spikes in usage. Through early May, Amazon’s stock was up 25% for the year. And the net worth of Bezos, already the world’s wealthiest person, had surged to $144 billion—a leap of $29 billion in a matter of months.
As is often with case with Amazon, the extraordinary results didn’t come without controversy. The company had to respond to the thousands of shadowy sellers who began price-gouging on its site. Then, on May 1, some Amazon workers participated in a nationwide “sickout” to protest what they described as inadequate safety precautions by the company in its facilities. Amazon terminated a handful of employees this spring who were outspoken in their criticism of the company’s safety practices. (In each case the company said the firings were because of violations of company policies, not in retaliation for speaking out.) In announcing its first-quarter results, Amazon said that in the second quarter it would spend some $4 billion or more on COVID-related expenses, including increased salaries for frontline workers, protective gear, and employee testing—enough to cancel out all of its expected operating profits for the period. For Amazon, it’s a small price to pay in order to get the focus back on execution.
Amazon’s reputation for speedy delivery has suffered a little during the crisis as well. Before the pandemic, the norm for most of the company’s Prime customers was one-day delivery and same-day for groceries. Since the pandemic hit, essential items like household staples and medical supplies have taken as many as four days, and nonessential items even longer. Amazon, which is relatively new to the grocery game—it bought Whole Foods in 2017—has been deluged with food orders, and in many cities the company simply hasn’t been able to offer enough delivery slots to fulfill demand.
Despite those stumbles, the consensus on Wall Street is that Amazon will emerge from the coronavirus crisis bigger and stronger than ever—and with consumers even more reliant on its breadth of products and services. “No company can handle the kind of surge in demand that Amazon can,” says Mark Mahaney, the veteran tech industry analyst at RBC Capital Markets. “When the pandemic is really over, the physical retail competition will be weakened—and Amazon comes out of this a winner.”
As always, Bezos is playing the long game. And it’s a strategy that has produced spectacular results. This year Amazon jumped three spots on the Fortune 500 list to No. 2—its highest ranking ever. Since the company first made the list in 2002 at No. 492, its market value has risen more than 22,000%—it was hovering at around $1.2 trillion in early May—and the company’s sales have grown an average of 28% annually. Studying the formula behind that stunning growth trajectory is key to understanding just how much more powerful Amazon may become over time.
Since the day Bezos founded Amazon in 1994, it has essentially been a data-driven company that just happened to do retailing. Over that quarter-century span, Bezos built perhaps the most sophisticated and successful data-powered corporation the world has ever seen. Amazon’s online retail business is powered by algorithms that scan buying patterns second by second and adjust what the company stocks in its vast warehouses, where to stock it, and the fastest way to deliver it.
Well before the pandemic, Amazon was using its digital might to increasingly insinuate itself into our lives. Some 150 million Prime members—a number that grew by 50 million in less than two years—order clothing, staples, and electronics from the e-commerce giant, watch original Prime Video movies and TV shows, and listen to music on Amazon’s streaming media channels. Even consumers who don’t actively use Amazon’s website to shop spend much of their digital lives using services like Netflix that run on Amazon’s ubiquitous AWS servers.
Now the pandemic has accelerated these trends more than anyone could have imagined—and America’s increased reliance on Amazon’s services is likely to stick. Some have even argued that Amazon is becoming a kind of corporate Red Cross, given its essential role in providing supplies for strapped local and state governments. Gene Munster, a partner at the research and investment firm Loup Ventures, told Fortune in a recent interview: “The U.S. would be in a tighter spot if it were not for Amazon. It is a national asset.”
More opportunities for expansion lie ahead. While Amazon dominates the U.S. e-commerce market with a 38% share, it accounts for only about 5% of total retail in the U.S. Pre-COVID-19, some 90% of all retail still occurred in brick-and-mortar stores. But until scientists discover an effective vaccine—and under the best-case scenario, that’s at least months away—many shoppers will be reluctant to return to malls and department stores. That means more will keep reaching for Amazon’s buy button. Even after the virus is contained, it’s easy to imagine that Amazon’s grocery business will continue to thrive. RBC predicts the segment, driven in part by online sales, will reach $88 billion in gross revenues by 2023—nearly double the 2020 level.
Amazon also sees an opportunity to use the virus to expand into new areas. Alexa, its magical voice genie, can now answer tens of thousands of COVID-19 questions such as, “Alexa, what do I do if I think I have the virus?” Or, “Alexa, give me tips for cleaning and disinfecting my home.” The company has even patented a technology that will enable Alexa to recognize the sound of a cough. How long before Amazon enters telemedicine? (It’s already offering its Amazon Care telehealth service to its Seattle employees.)
At the same time, Bezos has jumped headlong into the autonomous electric-vehicle race. He has invested billions to build a future in which packages will be delivered by self-driving vans, small bots rolling through neighborhoods, and drones buzzing to their destinations. One thing all those delivery options have in common? They’re impervious to the coronavirus. (Though potentially vulnerable to a computer virus.)
How did Amazon adapt so quickly to the pandemic? One of the company’s great strengths is that it’s run like a federation of independent nations, each with its own leader and citizens. In Seattle, where the company is headquartered, there’s no central corporate suite for the heads of all the business units. The execs are spread throughout the city, running their own operations. Bezos, of course, is the leader of the federation, and his word on important decisions is final. But his lieutenants have more latitude to move quickly, make decisions and investments, and pursue new innovations than is typical in today’s corporations.
From the outside, this structure seems like a recipe for disaster: fiefdoms operating in separate buildings scattered throughout downtown Seattle. But it works. And for one reason only. Bezos has inculcated his business with three bedrock principles that guide all decision-making: customer obsession, extreme innovation, and long-term management. Just about any CEO worth his or her stock options claims to follow some or most of these principles—so much so that they’ve become leadership clichés. Most, however, fail to execute them consistently and over long periods. Under Bezos, Amazon does.
Bezos’s secret is what he calls his flywheel, a conceptual engine that drives his three deeply seated values. At heart, the flywheel—a concept popularized by management guru Jim Collins—is a metaphor for a virtuous cycle. Rather than focusing on the competition, Amazonians spend their every working moment trying to make their customers’ lives better. One way is to lower costs. By doing that, Amazon increases the number of customers who visit Amazon.com. That attracts more independent sellers who want to reach the growing traffic on Amazon’s platform, which leads to more revenue for Amazon. That in turn leads to economies of scale, which help further lower prices for customers. The lower prices pull in still more customers. And the flywheel keeps turning and turning and turning.
It is this flywheel concept, which every Amazon manager knows by heart, that enables the giant corporation to operate as a federation of independent nations. Employees don’t have to wonder what their role is. Their job is to push the flywheel a little harder every day.
To keep building Amazon’s momentum, Bezos understood that his company had to continually renew each element of the flywheel by innovating. This meant Amazonians had to think imaginatively. They had to ask constantly what they could do to please customers and to attract more third-party sellers. “We are eager to pioneer and invent,” Bezos said last year. “This marries well with customer obsession, because customers are always dissatisfied even if they don’t know it, even when they think they’re happy. They always want a better way, and they don’t know what that will be. I warn people that customer obsession is not just listening to customers, it’s also inventing on their behalf.”
Every new innovation—Prime membership with one-day free shipping, free video and audio streaming, the Kindle, Fire TV, the Echo smart speaker, and Alexa—is designed to attract new customers and keep current ones happy.
As for being long-term oriented, Bezos has always known that building and maintaining a flywheel is a long, hard slog. All of Amazon’s major innovations—from the Kindle to AWS to the Echo—were many years in the making. Even when Amazon failed, as in the case of its late-to-market and mediocre Fire Phone, it kept innovating. Bezos felt deeply that failures were inevitable but even flops might pay off in the long run. Some of the learning from the failed Fire Phone, for instance, ended up in the Echo.
The relentlessness of Amazon’s push for efficiency and dominance has drawn accusations that the company has at times crossed anticompetitive lines. In late April, the Wall Street Journal published an investigative report alleging that Amazon had used inside information about sellers on its platform to develop competing products and then undercut the vendors on price. That prompted Congress to request that Bezos testify before the House Judiciary Committee. Amazon has said it is cooperating with the committee, but it is not clear whether Bezos will agree to testify. In response to the Journal article, Amazon said that using pricing data to undercut vendors would violate its policies and that it has launched an internal investigation.
Over the past decade, Bezos has taken the flywheel concept to an even higher level. Amazon is now applying big data, A.I., and machine learning to the operation at an unprecedented rate—to make it spin even faster on its own. This capacity is what helped Amazon respond so swiftly to the pandemic. In his 2016 shareholder letter, Bezos explained the power of such models: “Machine learning drives our algorithms for demand forecasting, product search ranking, deals recommendations, merchandising placements, fraud detection, translations, and much more.”
Think of this new iteration as the A.I. flywheel. The tens of thousands of engineers, data scientists, and programmers whom Bezos has hired have made the A.I. flywheel a learning machine, a cyber contraption with its own intelligence that takes all the data that Amazon collects on its customers and then analyzes it in minute detail. The machine makes decisions about what items to purchase, how much to charge for them, and where in the world to stock them. As Jeff Wilke, CEO of Amazon’s worldwide consumer division, explains: “In the old days we used data to help make decisions, but humans still made the ultimate decisions. Part of what we’re doing now with machine learning is taking some of the most repetitive intellectual processes and eliminating the requirement for human decision-making. We are able to close the loop so humans no longer have to decide. We place buy orders for millions of items automatically.”
Even scarier for its competitors is how much smarter Amazon’s algorithms may get from all the pandemic-fueled activity. Unlike businesses that are cutting budgets to stay afloat, Amazon is built to optimize in a crisis. It will almost certainly emerge on the other side delivering better service, at lower prices, to its customers. And the flywheel will keep on turning.
Leia o artigo da Fortune na integra >>
[/av_toggle]
[/av_toggle_container]
[/av_three_fifth][av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[/av_section]
[av_section min_height='' min_height_px='500px' padding='default' shadow='no-shadow' bottom_border='no-border-styling' bottom_border_diagonal_color='#333333' bottom_border_diagonal_direction='scroll' bottom_border_style='scroll' scroll_down='' custom_arrow_bg='' id='' color='main_color' custom_bg='' src='' attach='scroll' position='top left' repeat='no-repeat' video='' video_ratio='16:9' video_mobile_disabled='' overlay_enable='' overlay_opacity='0.5' overlay_color='' overlay_pattern='' overlay_custom_pattern='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av_element_hidden_in_editor='0']
[av_one_third first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_image src='https://www.aese.pt/wp-content/uploads/2020/12/Value-Killers_AESEinsight_3DEZ.jpg' attachment='68178' attachment_size='full' align='center' styling='' hover='' link='manually,http://www.amazon.com/Value-Killers-Acquisitions-Companies-Billions-ebook/dp/B07TPJ6TSX/ref=sr_1_1?dchild=1&keywords=nuno+fernandes+mergers&qid=1606747882&sr=8-1' target='_blank' caption='' font_size='' appearance='' overlay_opacity='0.4' overlay_color='#000000' overlay_text_color='#ffffff' animation='no-animation' admin_preview_bg=''][/av_image]
[av_heading tag='h3' padding='10' heading='Nuno Fernandes ' color='' style='blockquote modern-quote' custom_font='' size='' subheading_active='subheading_below' subheading_size='15' custom_class='' admin_preview_bg='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av-medium-font-size-title='' av-small-font-size-title='' av-mini-font-size-title='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='']
Professor de Finanças do IESE Business School
[/av_heading]
[/av_one_third][av_three_fifth min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_textblock size='' font_color='' color='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
A crise atual criou uma oportunidade única para novas aquisições e consolidações.No entanto, se a história antiga se repetir, muitos CEOs continuarão a embarcar em fusões e aquisições que provavelmente prejudicarão a sua organização.
A evidência passada é clara: a maioria das fusões fracassa. Elas destroem valor acionista e custam biliões às empresas. Importa sublinhar que este não é um fenómeno aleatório. Encontram-se padrões recorrentes em muitas fusões desastrosas. E, todavia, há soluções para que os CEOs e C.A. aumentem as hipóteses de sucesso nas fusões ou aquisições a que se abalancem.
Inscreva-se na sessão ALP online de dia 9 de dezembro, com Nuno Fernandes e saiba algumas das orientações práticas que abordou no seu livro, mais recente: “The Value Killers: How Mergers and Acquisitions Cost Companies Prevent It”.
[/av_textblock]
[av_toggle_container initial='0' mode='accordion' sort='' styling='' colors='custom' font_color='#f37421' background_color='#dcded9' border_color='']
[av_toggle title='Value Killers ' tags='']
In a business climate marked by escalating global competition and industry disruption, successful mergers and acquisitions are increasingly vital to the growth and profitability of many corporations. If history is any guide, 60 to 70 per cent of new mergers will fail – and will destroy shareholder value. To date, analyses of the M&A failure rate tend to focus on individual causes – e.g., culture clashes, valuation methods, or CEO overconfidence – rather than examining the problem holistically. The Value Killers is the first book based on a holistic analysis of successful and unsuccessful transactions. Based on research, interviews with top executives, and case studies, this book identifies the key causes of failures and successes and offers prescriptions to increase the odds that future transactions will deliver all the anticipated synergies.
The Value Killers offers practical advice in the form of 5 Golden Rules. These rules will help managers and boards to ensure that target companies are properly valued; potential synergies and risks are identified in advance; checks and balances are installed to make sure that the pros and cons of the transaction are rationally and objectively evaluated; mechanisms are created that will trigger termination of bad deals; and obstacles to successful post-merger integrations are assessed (and solutions developed) before the deal closes. Each chapter includes questions for executives considering future M&As to allow them to see whether they are on the right track or not.
Compre o livro aqui >>
[/av_toggle]
[/av_toggle_container]
[/av_three_fifth][av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[/av_section]
[av_section min_height='' min_height_px='500px' padding='default' shadow='no-shadow' bottom_border='no-border-styling' bottom_border_diagonal_color='#333333' bottom_border_diagonal_direction='scroll' bottom_border_style='scroll' scroll_down='' custom_arrow_bg='' id='' color='main_color' custom_bg='' src='' attach='scroll' position='top left' repeat='no-repeat' video='' video_ratio='16:9' video_mobile_disabled='' overlay_enable='' overlay_opacity='0.5' overlay_color='' overlay_pattern='' overlay_custom_pattern='' av-desktop-hide='' av-medium-hide='' av-small-hide='' av-mini-hide='' av_element_hidden_in_editor='0']
[av_one_third first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_image src='https://www.aese.pt/wp-content/uploads/2020/12/Constança_AESEinsight.jpg' attachment='68179' attachment_size='full' align='center' styling='' hover='' link='manually,https://www.linkedin.com/in/constan%C3%A7a-cacela-497a84ab/' target='_blank' caption='' font_size='' appearance='' overlay_opacity='0.4' overlay_color='#000000' overlay_text_color='#ffffff' animation='no-animation' admin_preview_bg=''][/av_image]
[av_heading heading='Constança Cacela ' tag='h3' style='blockquote modern-quote' size='' subheading_active='subheading_below' subheading_size='15' padding='10' color='' custom_font='' av-medium-font-size-title='' av-small-font-size-title='' av-mini-font-size-title='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
Director, RD Analytical Development, Hovione e Alumna do 73º PDE - Programa de Direção de Empresas da AESE Business School
[/av_heading]
[/av_one_third][av_three_fifth min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_textblock size='' font_color='' color='' av-medium-font-size='' av-small-font-size='' av-mini-font-size='' admin_preview_bg='']
Sempre fui fascinada pelo estudo, pela exploração e pela resolução de problemas. Sem surpresas, a ciência foi o caminho traçado durante vários anos. Mais tarde, desenvolver os outros e liderar equipas, levando ao alcance de objectivos comuns, tornou-se a minha paixão profissional. Antes de iniciar o PDE – Programa de Direção de Empresas da AESE, sentia o desejo de voltar a estudar e de percorrer caminhos de pensamento diferentes e desafiantes, além de que reconhecia a necessidade de desenvolver determinadas competências. Procurava algo de diferente, não só que me habilitasse de ferramentas para a excelência do desempenho profissional, mas que também me desenvolvesse enquanto ser humano. Fui aconselhada a consultar os programas da AESE. Na minha pesquisa, houve algo que me cativou e me fez escolher o PDE: “a arte de gerir a incerteza”, vinha escrito numa das brochuras. Seguiu-se a entrevista com o Professor Jorge Ribeirinho Machado, director de programa. Gostei da forma como avaliou as minhas necessidades e motivações e fiquei fascinada pelo conteúdo do curso – era uma mão cheia de possibilidades de saber que estavam à minha disposição.
[/av_textblock]
[av_toggle_container initial='0' mode='accordion' sort='' styling='' colors='custom' font_color='#f37421' background_color='#dcded9' border_color='']
[av_toggle title='O sucesso das empresas é resultado do comportamento humano' tags='']
Hoje, terminado o PDE, posso afirmar que foi uma experiência transformadora. A possibilidade de interagir com pessoas de áreas e experiências tão diversas, além de imensamente enriquecedor, mostra-nos que existe uma variedade de abordagens e formas de pensamento tão certas, quanto diferentes, das nossas. Os trabalhos de grupo e debates revelam a riqueza do pensamento humano e a relevância de cada um na equipa. O debate em grupo sempre antecedido pela reflexão individual dos casos: entrar dentro das personagens, reflectir sobre elas, viver os seus desafios nas suas empresas. As personagens de cada caso não são mais do cada um de nós nas suas funções, com os mesmos desafios, os meus dilemas nas diferentes àreas de uma empresa: das finanças ao factor humano, passando pelo marketing, operações e política de empresa. E assim, ao reflectir sobre o caso, sobre cada uma delas, reflectimos sobre nós próprios e as nossas escolhas no âmbito da nossa vida profissional, na nossa empresa. O caso faz-nos escolher possíveis caminhos, em direcção a soluções, promovendo o pensamento estratégico.
O conteúdo programático e o método de ensino de pouco serviam se não estivessem entregues a conjunto de professores extraordinários. A robustez do seu conhecimento, que toca tantas àreas diferentes, aliada à sua genuína vontade de partilhar e de nos desenvolver enquanto líderes, é verdadeiramente diferenciador.
Referi que o PDE foi uma experiência transformadora. Além de ter aumentado o meu conhecimento em áreas chaves para o meu desempenho profissional, sinto que me deu ferramentas que me permitem tomar decisões, no meu dia-a-dia na empresa, mais sustentadas e num curto espaço de tempo. Este era um dos objectivos: com poucos dados, e sem ser uma especialista em determinada área, a título de exemplo contabilidade ou finanças, saber o que é relevante, focar-me no essencial e juntar os dados que me permitem a tomada de decisão. Tornei-me mais confiante com as minhas escolhas, sei melhor justificá-las porque estão bem sustentadas, e sinto que aumentei bastante o meu pensamento estratégico. Essencial na minha função é também a habilidade para a identificação de problemas no campo de operações: onde estão os gargalos de determinada actividade? Como faço mais, com menos esforço e sem aumentar recursos? Hoje consigo fazer avaliações rigorosas e análises não meramente apoiadas em percepções que, podendo não estar erradas, sentia sempre alguma dificuldade em justificar.
Termino com o que me é mais caro e sempre mais desafiante: o factor humano, as pessoas e o seu potencial. Seja qual for a àrea de saber, o caso ou o professor, é na humanidade presente em tudo o que se faz e ensina na AESE que reside a diferenciação da escola. Colocando o ser humano no centro, vamos desenvolvendo as nossas competências enquanto líderes. O que aprendi nesta àrea, aquando da discussão dos casos, através de partilha sincera de todos nós, é-me difícil quantificar. Sei sim que desenvolvi, que tenho hoje ferramentas que não tinha.
Trabalho para uma empresa cujo ADN é a ciência e a inovação, onde as competências técnicas são sem dúvida muito importantes. Contudo, é também amplamente reconhecido que o seu sucesso, e o das empresas em geral, por mais tecnológicas que sejam, é resultado do comportamento humano, das decisões e opções tomadas por cada um dos seus líderes em todos os níveis da organização. Líderes que desenhem caminho na procura de soluções inteligentes para desafios cada vez maiores. Líderes que marcam o mundo, um mundo de saber.
[/av_toggle]
[/av_toggle_container]
[/av_three_fifth][av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[/av_section]
[av_one_third first min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[av_magazine link='category,72' items='5' offset='5' tabs='aviaTBtabs' thumbnails='aviaTBthumbnails' heading_active='aviaTBheading_active' heading='Leia e veja outras edições' heading_link='post,64984' heading_color='orange' heading_custom_color='#ffffff' first_big_pos='top' admin_preview_bg='']
[/av_one_third]
[av_one_third min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[av_magazine link='category,226' items='6' offset='no_duplicates' tabs='aviaTBtabs' thumbnails='aviaTBthumbnails' heading_active='aviaTBheading_active' heading='Alumni AESE ' heading_link='post,8847' heading_color='orange' heading_custom_color='#ffffff' first_big_pos='top' admin_preview_bg='']
[/av_one_third]
[av_one_third min_height='' vertical_alignment='' space='' custom_margin='' margin='0px' padding='0px' border='' border_color='' radius='0px' background_color='' src='' background_position='top left' background_repeat='no-repeat' animation='' mobile_breaking='' mobile_display='']
[av_hr class='invisible' height='70' shadow='no-shadow' position='center' custom_border='av-border-thin' custom_width='50px' custom_border_color='' custom_margin_top='30px' custom_margin_bottom='30px' icon_select='yes' custom_icon_color='' icon='ue808' font='entypo-fontello' av-small-hide='aviaTBav-small-hide' av-mini-hide='aviaTBav-mini-hide' admin_preview_bg='']
[av_magazine link='event-categories,290' items='4' offset='1' tabs='aviaTBtabs' thumbnails='aviaTBthumbnails' heading_active='aviaTBheading_active' heading='Agenda AESE ' heading_link='post,8847' heading_color='orange' heading_custom_color='#ffffff' first_big_pos='top' admin_preview_bg='']
[/av_one_third]